Unified Time Server Total Solution for Medical Industry
Hospital-wide Unified Time Reference - Medical Grade Highly Reliable Timing System
Through the design of BeiDou/GPS traceability, multi-protocol timing and multi-level redundancy, it builds an informationized unified time system throughout the whole hospital to guarantee the safety, traceability and auditability of medical services.
With the in-depth advancement of hospital informatization, business platforms such as HIS, EMR, LIS, PACS, monitoring system, surgical anesthesia system, etc. rely heavily on accurate and unified time labels. Time is not only the basis for the sequence of medical processes, but also an important foundation for the realization of traceability of electronic medical records, audit records, guardianship data, imaging examinations, security systems, and so on.
However, time inconsistencies are common in actual hospital operations: different servers and systems may use different time sources; time drifts between devices due to network delays, manual settings, unconfigured NTP/PTP, etc.; and a few older devices even rely on built-in crystals for long term operation, where the deviations accumulate even more significantly. These issues pose a range of potential risks to hospitals, including: these discrepancies can lead to conflicting medical records, mismatched imaging and test data, misaligned monitoring curves and surgical events, and difficulties in fault localization and audit checks.
With the clear requirements for "unified time and traceability" put forward by compliance standards such as electronic medical records, interconnection and level protection, hospitals urgently need to construct a set of Independent, secure, stable and hospital-wide unified time synchronization systemto ensure healthcare business continuity, data trustworthiness and audit compliance.

Overall construction goals
Harmonization of time benchmarks across the hospital
All business systems, servers, terminals, monitoring equipment, and imaging equipment share the same time source.
Meet medical regulatory and audit requirements
Electronic medical records, interconnectivity, and equivalency level protection all require time consistency and traceability.
Highly accurate and scalable
It is also compatible with NTP / PTP / 1PPS / IRIG-B to meet different service requirements from milliseconds to microseconds.
Multiple redundancy design
Time sources, timing devices, network links, and client policies are fault-tolerant to ensure that services are not affected by a single point of failure.
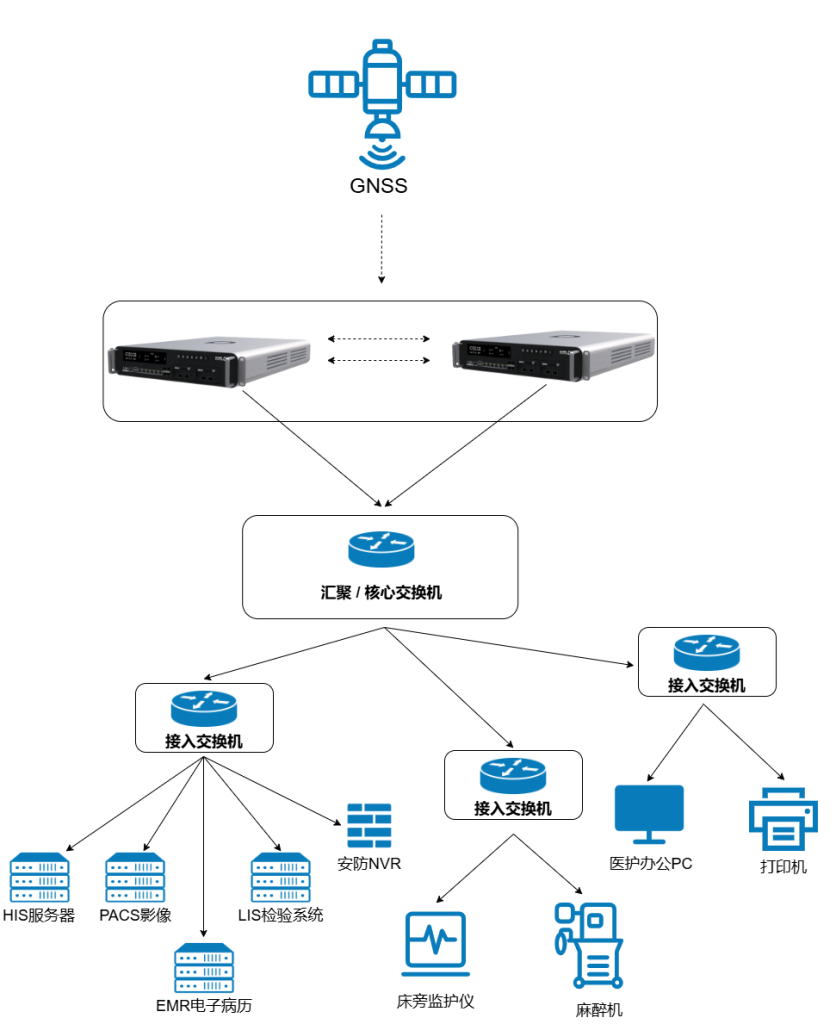
Unified Timing System Architecture for Healthcare Industry (Source - Web - End - Table)
1. Time source (source)
Standard UTC/Beijing time is acquired using Beidou or Beidou+GPS dual mode;
Built-in OCXO, Rubidium, or Cesium master clock maintains high-precision timekeeping for long periods of time in the event of star drop or interference.
2. Time networks (nets)
Deploy two to three (or more) medical-grade time servers in the server room as the hospital-wide primary time source;
Provides NTP, PTP, and SNTP authorization services to each network segment;
Large hospitals can combine PTP-enabled core/aggregation switches to build a BC/TC architecture to improve PTP accuracy and stability.
3. Access terminal (end)
Business servers such as HIS, EMR, LIS, PACS, imaging workstations, etc. are synchronized via NTP/Chrony;
Medical devices, such as Mindray monitors, are directly timed via SNTP;
High-precision scene devices can be accessed via PTP, 1PPS, IRIG-B, etc.
4. Visualization clocks (tables)
Deploy networked sub-clocks in areas such as wards, corridors, nurses' stations, operating rooms, and emergency rooms;
All spreadsheets are aligned with the system time to ensure uniformity in the time seen by healthcare professionals and patients.

Multi-protocol timing capability compatible with new and old devices
In hospitals, there is a wide range of equipment ages, and old and new equipment coexist, so time servers need to support multiple protocols and interfaces:
NTP / SNTP
- Covers most IT servers, PCs, Linux/Windows systems, network printers and more;
- SNTP is compatible with mainstream monitors, anesthesia machines and other bedside devices.
PTP (IEEE 1588)
- For high-precision scenarios, such as operating room audio and video, image interconnection, and research platforms;
- It can be combined with switches that support hardware timestamping to the microsecond and even nanosecond level.
Serial TOD/ 1PPS / IRIG-B
- For older large equipment or research equipment, accessed via coaxial cable/terminal;
- Highly resistant to interference and does not rely on IP networks.
Three ways to seamlessly integrate into hospital construction
New construction / expansion of hospital intellectualization project
- As the core device of the "hospital-wide unified clock system" or "time synchronization subsystem";
- Tenders are invited together with weak electrical works, computer room works and integrated cabling.
Information System Upgrade / Integration Project
- Serves as supporting infrastructure for HIS/EMR/LIS/PACS upgrades;
- Planning with the MDI (Medical Device Integration) platform, with "time harmonization" as a prerequisite for integration.
Section-specific projects
- PTP and high-precision time systems are first deployed locally in the department to meet the scenarios of high-definition surgical video and convergent monitoring;
- Later, it will be gradually extended to the whole hospital to realize "one set of equipment, shared by multiple departments".
Typical Deployment Patterns
goal
- Hospital-wide servers,PC, key equipment time uniformity, error control within milliseconds;
- Eliminate single points of failure:: Any one time server is down or antenna fails, the service terminal is switched without sense and no time jump occurs;
- Meet the basic needs of electronic medical record auditing, health insurance reconciliation, and log tracing;
- Program Simplicity, Information Section It can be maintained by 1 or 2 people.
Core idea:
- Deployment of 2 units in the data center server room Medical-grade time servers(both active);
- The two servers are connected to separate GNSS antennas (it is recommended that they be located in separate locations to protect against lightning strikes or shading), which are connected to the hospital's core/aggregation switches as two separate primary time sources (Stratum 1) below;;
- All servers, PCs, network video platforms, surveillance NVRs, and SNTP-enabled monitors are unified and point to the IP addresses of these two servers at the same time;
- There is no need to change the existing service topology, just add two new Time Service IPs to the existing network.
Utilizes NTP's native "clock selection algorithm".
- Principle:NTP clients (whether Windows Time Service or Linux NTPd/Chrony) are inherently capable of handling multiple time sources.
- Advantage:When we populate the client with both server IPs, the client communicates with both servers at the same time. If one of them suddenly loses power or the satellite goes out of lock, the client's algorithms are based on theTime level (Stratum),Delay cap (a poem) Jitter Automatically recognizes the source as "untrustworthy" and smoothly eliminates it, using only data from another station.
Key Technology Points
The T830 clock server itself should be "stable".
- External: Use Beidou satellite as time source to ensure that the time is consistent with the national standard;
- Internal: With a time-keeping unit thermostat crystal, when the satellite signal is lost for a short period of time (e.g., 24 hours), the time deviation (drift) is very small, basically at the microsecond level, and does not affect business. If you choose the time-keeping unit rubidium species, even if you lose the satellite signal for a few months, you can do microsecond time deviation.
The T830's NTP concurrency should be adequate
- Small hospitals may be small, but with ward PCs, monitors, and printers, NTP clients can easily number in the hundreds;
- The time server needs to support "hundreds or thousands of devices asking for the time at the same time without getting stuck" to avoid the monitor reporting "time server not found" error.
T830 Compatible SNTP Devices
- Some monitors and anesthesia machines support SNTP, we just need to fill in the time server IP in their configuration;
- The time server is fully compatible with SNTP requests and does not need to be adapted separately.
The T830 provides a basic web-based management interface
- The Information Section can see the current satellite lock status, the time deviation of each NTP client, the status of the NTP Authorization Service, as well as the regular system resource monitoring, etc. in the browser;
- Check for "stars, deviations and services" on a daily basis, and see at a glance when things go wrong.
T830 reserved PTP/physical interface for upgrading.
- Although small hospitals can not use PTP microsecond precision, the device supports PTP, 1PPS/IRIG-B interfaces, etc. In the future, when upgrading imaging centers and operating rooms, there is no need to change the time server, but only need to turn on PTP in the side of the new equipment.
Implementation steps
For small hospitals, we recommend a "three-step process" that seeks toResults within a week(from program preparation to hospital-wide switchover, as determined by the rhythm of the hospital)
preparatory phase
- Determine the time server room location and GNSS antenna alignment (typically up on the roof or outside the room window);
- Reserve a service port and IP segment on the core switch;
- The Information Section makes a list of servers and critical systems that need to be synchronized (HIS/EMR/LIS/PACS, etc.).
on-line phase
- Install the time server and antenna, complete the star receiving debugging, and confirm the time is accurate;
- Start by configuring NTP on a non-core business server to verify synchronization;
- And then gradually expand to HIS, EMR, LIS, PACS, monitoring platform and other core systems;
- Finally, the department was notified to perform time source switching for some PCs and monitors during business-neutral hours.
Validation and handover
- Spot-check the time of multiple servers and terminals to ensure that deviations from the time server are within milliseconds or sub-milliseconds;
- Verify that "Order Time," "Charge Time," and "Report Time" are aligned through log matching;
- Handover of web management account to the Information Section, training on how to check status and simple troubleshooting.
Expected results after deployment in small hospitals
Smaller hospitals can quickly feel these changes after deploying a unified time server:
The log time "speaks consistently":Logs from different systems can be viewed in chronological order, making troubleshooting and responding to inspections easier.
Medical records, billing, testing, and imaging times are standardized:Doctors will no longer complain that "the report comes out at 8:05, but the doctor's order is not issued until 8:10, which is awkward to look at"; when issuing copies of medical records to the public, they will also be able to withstand more scrutiny.
The Information Section is even less likely to "take the blame":Many ambiguous issues (clinical says slow, financial says wrong) can be located quickly by harmonizing time and log chains and won't always fall on the information section.
Reserve space for subsequent upgradesWhen the hospital develops its business and needs to upgrade its smart wards, digital operating rooms, and remote consultation, the time system has already laid the foundation and can be smoothly upgraded by adding PTP and a small amount of equipment at the local level.
NTP base + PTP upgrades in key sections
We recommend a one-sentence strategy for building time systems in mid-sized hospitals:
"NTPs bottom out across the hospital and PTPs are upgraded first in key departments."
- All servers and general purpose terminals throughout the hospital continue to be NTP-based (similar to a small hospital);
- rightClear demand for high precisionFor departments (operating rooms, ICUs, and imaging centers), on the basis of the original time servers, the PTP capability is enabled, and a small number of PTP-enabled switches and terminal devices are used to tighten the accuracy from milliseconds to microseconds and nanoseconds.
The benefit of this is:
- No "one size fits all" reconfiguration of the network, with a manageable amount of modification and risk;
- The Information and Equipment Sections can pilot the program in one or two sections to run through the experience before gradually expanding it to the entire hospital.

- The server room is recommended to deploy at least Three clock servers (three devices can meet the minimum number of "bad clock rejection" requirements of the NTP algorithm, which greatly improves the anti-interference ability), support:
- Single BeiDou (optional BeiDou+GPS dual-mode) timing, built-in constant temperature crystal (OCXO)/Rubidium/Cesium clock for timekeeping;
- Simultaneously outputs NTP / PTP, TOD, 1PPS, 10M, IRIG-B and many other time sources;
- NTP service:Abandon the traditional VRRP virtual IP switching mode and adopt theClient-side multi-source concurrencyConfiguration. The core switches and business servers of the whole hospital point to the three time server IPs at the same time, and the client NTP algorithm evaluates and rejects the source with large deviation in real time, realizing millisecond-level senseless fault shielding.
- PTP service:Enabling IEEE 1588 BMCA (Best Master Clock Algorithm). The three devices are candidates for each other's master clock GM, and when the current master clock satellite is out of lock or fails, the switches and terminals within the network will automatically switch smoothly to the next optimal clock based on priority and clock quality, realizing seamless succession at the microsecond level."
- The master clocks can be used as time sources for each other, and can be automatically switched or alerted in the event of an abnormality.
The high accuracy of PTP depends on the hardware support of the switch (IEEE 1588 chip). Considering the high cost and risk of upgrading the hospital-wide core network, we propose to use thehybrid networkingStrategy:
- Hospital-wide backbone (NTP layer):The existing core and aggregation switches remain unchanged and continue to carry NTP traffic to meet the demand of 95% servers and terminals (milliseconds) across the hospital.
- High Precision Business Domain (PTP Layer):Deploying or upgrading in specific areas such as operating rooms, imaging centers, etc.PTP-enabled access layer switchesThe
- Scenario A (Leverage):If existing aggregation switches do not support PTP hardware timestamps, we use these high-precision regions as thePTP SiloThe time server's PTP port is physically connected directly to the area switch.physical bypassin the core network to avoid congestion in the core network interfering with PTP accuracy.
- Option B (New Construction):In new buildings, it is recommended that support be procured Boundary Clock (BC) mode aggregation switches for end-to-end full-link hardware marking.
- All-optical network surgical demonstration/recording system:Configure the PTP client for encoders and cameras that support the ST 2110 standard to realize the followingframe-level synchronizationIt is guaranteed that the multi-camera switching screen will not be torn or blacked out;
- Guardianship centralized platform server:Enable the PTP function for lower clock jitter to ensure that the high-frequency waveform data aggregated by multiple bedside devices are strictly consistent in timing, assisting doctors in accurate trend analysis;
- If the imaging equipment, such as CT / MR, supports PTP / IRIG-B, it is directly connected to the time server or PTP network.
Medium-sized Hospital Implementation Priorities and Considerations
The PTP protocol is extremely sensitive to network jitter
- Set the time server's PTP dedicated network portConnects directly to the access switch in the OR/imaging center, creating a separate physical link that does not pass through the busy hospital core network. This is the least expensive and most reliable way to achieve microsecond synchronization.
- If you must go through the backbone, you must configure all switches along the route for PTP messages (UDP port 319/320 or Layer 2 multicast) Highest priority QoS queueThis ensures that time messages are prioritized for "queue-jump" forwarding, minimizing queuing delays on older switches that do not support PTP.
Collaboration with business system vendors
- Prior to the deployment of the time system, it is recommended that the Information Section send out a uniform letter or meeting to notify the various HIS/EMR/LIS/PACS/Hand Anesthesia/Critical Care system vendors:
- The hospital will enable a unified internal time server (IP address provided);
- Require subsequent shelves, upgrades, after-sales priority to use this time source, and close the system hard-coded public NTP address. If possible, you can replace it with a domain name address, so that it will be more convenient and easy to modify the equipment later.
- Older systems that require configuration changes can be centralized through upgrade patches or maintenance windows.
Subclock and Section Display
- According to the "General Hospital Building Design Code" and "Electrical Design Code for Medical Buildings", it is appropriate to set up sub-clocks in the locations of registration, outpatient clinics, charging, waiting areas, operating rooms, ward corridors and so on.
- Medium-sized hospitals can directly connect the network sub-clock to the unified time network when they build or renovate the weak electricity project:
- Sub-clocks in wards and corridors are accessed via Ethernet/wireless, and are unified to retrieve the time from the time server;
- A large screen clock is available in the operating room to standardize the time with the surgical recording system.
Post-construction benefits of medium-sized hospitals
For medium-sized hospitals, an NTP + local PTP time system can bring:
- Overall pass rate increase
- Audit log consistency and data time traceability are more likely to meet standards in interconnectivity and electronic medical record review;
- "Synchronization of audio and video" in key sections
- Surgery video time and anesthesia records and monitoring data can be precisely aligned for clearer review after the fact;
- When ICU multi-parameter monitoring is centrally displayed, the waveforms are aligned so that "one is fast and one is slow" is not easily seen.
- Reduced operations and maintenance workload
- There is a unified monitoring interface (SNMP/API), and there are alerts for time anomalies, rather than waiting for business failures to be discovered;
- System/integrators come to the hospital to do upgrades, change servers, as long as the specification to access the time server can be, without repeated manual time adjustment.
Multi-level PTP + NTP coexistence, covering multiple hospital districts
The information system and network structure of this kind of hospitals are extremely complex, and a simple "one intranet NTP server" is far from enough, and it is necessary to constructHierarchical, multi-domain, high precision time network with self-healing capabilityThe
- Hospital-wide harmonization of UTC traceability chain: From BeiDou/GPS → Core PTP Master Clock → Boundary Clock/Transparent Clock → Servers and Devices → Audit Log.
- NTP and PTP Coexistence::
- NTP service covers most servers and terminals (simple and compatible);
- The PTP service covers critical domains that require microsecond/nanosecond accuracy.
- Multi-campus, multi-master clock synergy::
- Each hospital district deploys a local PTP master clock (T-GM), which is uniformly fetched from the same set or class of GNSS/PRTC sources and backed up by each other;
- Time consistency is maintained between hospitals through dedicated lines or MPLS VPNs.
- High Availability + Ops Visualization::
- Dual master clock, dual power supplies, dual network port redundancy;
- A complete monitoring interface and large visualization screen turn time into an observable resource.

BeiDou satellite time source with T830 model master clock layer
Multimode Redundant Architecture
- The master clock clusters deployed at each campus use theIndependent RoutingPolicies. Avoid the risk of a single point of failure (such as ARP spoofing or broadcast storms) with a single virtual IP.
- The core network layer establishes Layer 3 routing connections directly to multiple physical clocks, ensuring that even if an access switch fails, time services can still be delivered over other links.
Multi-campus GNSS / Beidou Timing
- At least one set of BeiDou/GPS antenna + T830 model master clock device per campus;
- For important hospitals, consider reserving ePRTC capability (Enhanced Timekeeping) to maintain high accuracy for long periods of time when GNSS is disturbed.
Model T830 Master Clock Device (Class T-GM)
- Supports PTP (IEEE 1588v2) Multiple Profile (e.g., telecom, etc.) and can be configured for multiple PTP domains;
- It also provides NTP services to time devices and systems that do not support PTP;
Network PTP distribution layer (BC / TC)
Core switch as T-BC (border clock)
- Each hospital core switch takes the PTP time from the local master clock and becomes upstream of the downstream;
- Forward PTP messages between different VLANs/subnets while correcting its own dwell time.
Aggregation/access switch as T-TC (transparent clock)
- Adding delay compensation to PTP messages traversing itself keeps the overall error to microseconds or less;
- Transparent to other business messages and does not change existing business logic.
multi-domain strategy
- Define different PTP domain numbers and priorities for surgery centers, imaging centers, and research clusters;
- Avoiding interference between different business domains while ensuring a high degree of time consistency within their respective domains.
Terminal and Business System Layer
Scientific Computing / AI Domain
- Nanosecond control is achieved using a network card and PTP client that supports hardware timestamping;
- Ensure that training logs, inference logs, and business logs are strictly aligned on the timeline to facilitate performance tuning and problem localization.
High-end medical device domain
- Direct access to high-precision time for imaging equipment, radiotherapy equipment, surgical robots, etc. that support PTP or IRIG-B;
- For older devices that only support NTP / SNTP, utilize the clock server NTP function compatibility.
Traditional information systems domain
- HIS / EMR / LIS / PACS / Manual Anesthesia and other systems continue to be dominated by NTP;
- The database and application logs, combined with the precise timing of the PTP domain, establish theHarmonization of timelines across systemsThe
Typical landing scenarios in large hospitals
Scenario 1: Operating Room "Black Box"
- There are key points such as patient admission, induction of anesthesia, skinning, critical operations, and end shutdown:
- The time of the event as recorded by the surgical anesthesia system;
- Waveforms and alarm times of the monitor;
- Time for surgical video taping;
- The time displayed on the electronic screen at the entrance to the operating room.
- Under the Unified Time System, these times are perfectly aligned, and in the event of a surgical accident or dispute, the hospital can provide a complete and credible timeline and improve its ability to prove its case.
Scenario 2: Imaging Center + Regional Imaging Platform
- Our CT / MR / DR / DSA equipment and PACS images all use a uniform time;
- When exchanging images with higher hospitals or regional imaging platforms, the examination time, reading time, and teleconsultation time are consistent;
- It is conducive to reflecting "data traceability, shareability and reusability" in the interoperability assessment.
Scenario 3: Research and AI Platforms
- When hospitals build their own research computing/AI platforms (e.g., imaging AI, pathology AI, in-hospital large model training):
- Harmonized time ensures consistent timestamps across different data sources (HIS, EMR, exams, procedures, follow-ups);
- Model training logs, inference logs and source data events can be one-to-one correspondence, which is convenient for scientific reproduction and auditing.
Operations and monitoring design: making time "visible and manageable"
For the Information Technology Section, the time system is not a black box that can be installed and forgotten, but an infrastructure that needs to be integrated into the daily operation and maintenance system.
Satellite timing status
- Number of visible/locked satellites (Beidou/GPS display);
- Current UTC deviation, antenna short/break alarm.
timing service status
- NTP service process health, request volume, number of clients;
- PTP instance status (domain number, tier, master/standby switchover situation), deviation and jitter profiles.
Device Resource Status
- CPU, memory, and storage utilization;
- Whether the Holdover state is on.
Alarms and logs
- Time deviation over threshold alarm (e.g. abnormal jitter at a certain time);
- GNSS lost stars, switching, antenna failure;
- Master-standby switchover, reboot, configuration changes.
Procurement and construction proposals
Why do I need to build my own time server instead of continuing to use public NTP?
- compliance requirement::
- Systems such as electronic medical records, interconnectivity, and health care management require complete and credible time records of data operations;
- With public NTP, the hospital has no control over its stability and cannot be held legally responsible for the correctness of its timing.
- safety requirement::
- Equal Protection 0 Emphasizes internal and external network boundary protection and minimum exposure, and the core business network is not suitable for long-term external connection to the public network time source;
- The self-built time system can be fully closed loop on the intranet.
- business continuity::
- The hospital can't do anything when the public NTP is interrupted or the deviation increases;
- Self-built systems can be redundant across multiple sources and server rooms, and you can troubleshoot and fix problems yourself.
Inputs mainly include:
- Time server equipment (2 for small hospitals, 2 for medium and large hospitals according to the hospital district);
- GNSS antenna fixing and feeder (coaxial cable) threading alignment;
- Switch increments with PTP support (critical domains only);
Outputs and benefits:
- Risk reduction
- In medical disputes, the chain of time evidence is more complete, reducing the passivity caused by the "record time mess";
- Audits, inspections, and flight checks are easier to pass when the logs and times match up.
- Efficiency gains
- Faster troubleshooting: logs can be strung together by time, rather than looking at separate tables;
- Cross-system and cross-division data analysis and research projects are smoother.
- Sustainable development
- To build a good "time foundation" for future digital upgrades (smart wards, operating room upgrades, teleconsultation, research platforms) in advance, avoiding the need to rebuild the underlying layers in the future.
Frequently Asked Questions (FAQ)
Why do we need to be on a dedicated time server when our hospitals can look at the time now?
Now most of the time from their respective computers, equipment comes with the table, who is fast and who is slow no one cares. When something really goes wrong, such as a medical dispute or an audit, you realize that "everyone's watch is different". The role of the time server is to allow the hospital from "each look at their own table" to "all the people uniformly look at the same table", and the time of this table has a satellite and specialized equipment "endorsement ".
Do I have to change all the equipment in the hospital to PTP?
PTP is used in two main types of scenarios:
- A digital operating room that meets new standards:If your new building utilizes an IP-based 4K video transmission solution such as the ST 2110, PTP is a must-have infrastructure.
- High-value scientific data collection:For example, ICU critical care data centers that need to do multimodal AI training.
Our recommendation is that NTP is sufficient for general business, and PTP capability is pre-built for areas involving "video streaming" and "big data research".
What if there is a lot of stock and old equipment that can't be changed?
It's not necessary at all, nor is it recommended. We followthe twenty-eight principle (in economics)::
- 80%'s general purpose areas (office, clinic, nurse's station):Continue to use the NTP protocol with your existing network equipment. there are no special requirements for NTP on the switch. your old equipment is fully compatible.
- Critical areas of 20% (operating rooms, research platforms):If these areas require microsecond accuracy and existing switches do not support the PTP hardware feature, we have two low-cost options:
- Software PTP mode:Running PTP on unsupported switches, the accuracy is less than microseconds, but still better than NTP (about 10-100 microseconds), and in non-core backbone links, utilizing the software PTP mode allows forSub-milliseconds (hundred microseconds)Synchronization is sufficient for general HD audio and video needs without hardware replacement.
- Localized additions:Only in the top of these cabinets to add a small PTP access switch (cost is very low), to build a small "high-precision time island", do not need to move the entire hospital backbone network.
The overall idea isCompatible with the stock, take care of the increment, progressive evolution.
If I don't configure a virtual IP (VIP), will the hospital's time be messed up when one of the time servers fails or the satellite goes down?
Not at all, but rather more stable.Conventional "master-standby" mode (VIP) often results in time "jumps" or short-term interruptions at the moment of switchover. We use a more advancedMultiple machines in parallelMode:
- Terminal omniscient:Critical hospital equipment and servers will be in communication with all time servers at the same time.
- Automatic Preferences:The device's internal algorithm compares the quality of several time sources in real time. If one of the servers has a deviation in time due to satellite interference (large Stratum) or is completely down, the end device **"smoothly ignores "** it and continues to use other normal servers.
- Seamless transition:The entire process is completely transparent to the business application and there is no "switching action", thus eliminating the risk of "switching shock".
What does this system have to do with what we're doing now with equipoise, connectivity, and electronic medical record review?
Simply put, it provides a "reliable timeline" for these tasks.
- The EHR specification requires that all operations be accurately time-stamped;
- Equipoise 0 Emphasizes log auditing, event tracing, and the need for time consistency;
- The interoperability assessment requires data to be reconciled and reproducible in a harmonized manner across different systems.
Without a unified time, these can only be "on paper to meet the standard"; with a unified time, in order to really do "clear, right, check".